Interventional Radiology: Minimally Invasive Alternative to Surgery
Our nationally recognized interventional radiologists within the UCSF Radiology and Biomedical Imaging Department have extensive experience and success using minimally invasive surgical techniques to treat patients with a wide variety of disorders. These techniques are less invasive than open surgery. Therefore, recovery is faster with generally less discomfort and fewer associated complications. All of our interventional radiologists are board-certified radiologists with advanced training in image-guided procedures and subspecialty certification from the American Board of Radiology in vascular and interventional radiology.




Why choose Interventional Radiology at UCSF
- Most advanced techniques and state-of-the-art imaging equipment with reduced X-ray doses
- Pioneering work in the treatment of various diseases
- Patient–centered care
- Minimally invasive interventional techniques, resulting in shorter recovery time for patients, less time in the hospital, and less pain as a side effect of the procedures when compared with open surgery
- Specially designed interventional radiology clinics that optimize patient evaluation and treatment
Interventional Radiology Issues We Address
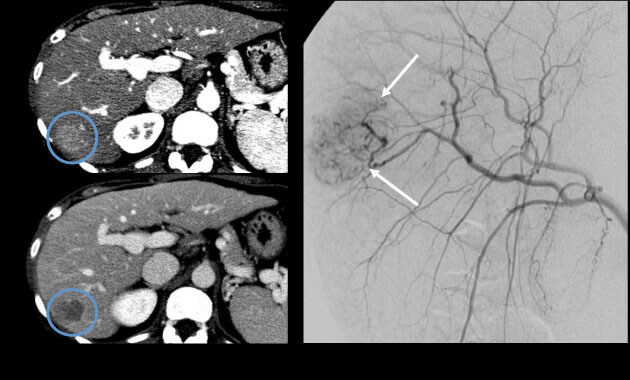
Interventional Oncology
- Conditions: Liver cancer (hepatocellular carcinoma, cholangiocarcinoma), liver metastases (colon or rectum, neuroendocrine, breast, other), kidney cancer, lung cancer, adrenal tumors
- Services: Embolization, chemoembolization, Yttrium-90 (90Y) radioembolization, microwave ablation, cryoablation, alcohol ablation, biopsies
Men’s Health
- Conditions: Benign prostatic hyperplasia (BPH), varicocele
- Services: Prostate artery embolization (PAE), varicocele embolization, varicoceles male infertility treatment
Women’s Health
- Conditions: Uterine fibroids, adenomyosis, pelvic congestion syndrome, infertility
- Services: Uterine artery / uterine fibroid embolization (UAE / UFE), High-intensity focused ultrasound (HIFU), gonadal vein embolization, fallopian tube recanalization
Venous Disease
- Conditions: Superficial venous disease and varicose veins, deep venous thrombosis, pulmonary embolism, May-Thurner syndrome, Paget-Schroetter syndrome
- Services: Varicose vein ablation, sclerotherapy, inferior vena cava (IVC) filter insertion and removal, thrombolysis, angioplasty, stenting, angiovac thrombectomy
Dialysis Access Interventions
- Conditions: Hemodialysis access, access malfunction
- Services: Dialysis access catheters, maintenance of dialysis fistula / graft patency (de-clot, thrombolysis, angioplasty, stenting)
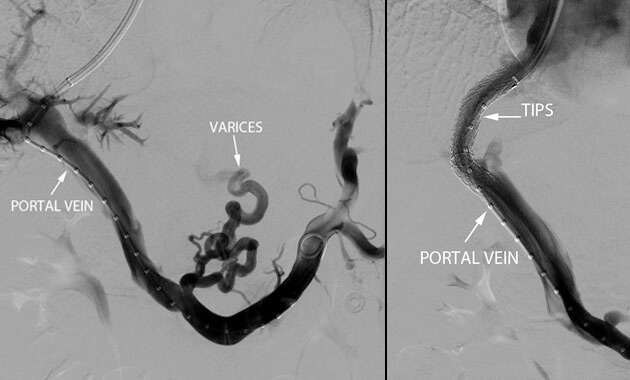
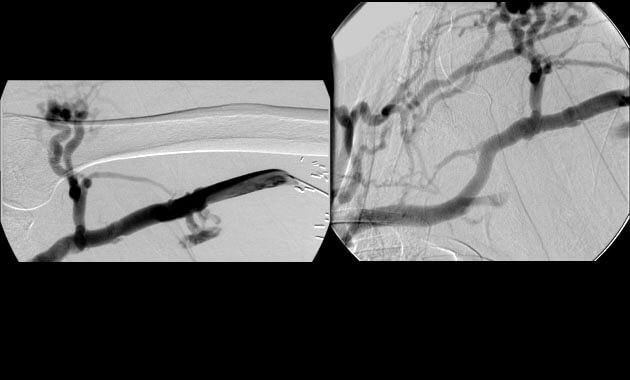
Portal Hypertension
- Conditions: Portal hypertension, esophageal varices, gastric varices, variceal bleeding, ascites, portal vein thrombosis, Budd-Chiari syndrome
- Services: Transjugular intrahepatic portosystemic shunt (TIPS), Balloon-assisted retrograde transvenous obliteration (BRTO), portal vein recanalization, paracentesis, abdominal PleurX placement
Genitourinary Interventions
- Conditions: Hydronephrosis, ureter obstruction, angiomyolipoma (AML)
- Services: Nephrostomy, ureteral stenting, embolization
Billiary Tract Disease
- Conditions: Bile duct obstruction, bile leak, cholecystitis
- Services: Percutaneous transhepatic biliary drainage (PTBD), cholangioplasty, stenting, cholecystostomy
Liver, Kidney, Pancreas, and Lung Transplant Interventions
- Conditions: Rejection, infection, abscess, vascular problems (stenosis, bleeding), bile duct obstruction, bile leak, hydronephrosis, ureter obstruction, urine leak, pleural effusion
- Services: Angiography, venography, angioplasty, stenting, transjugular liver biopsy, biliary drainage, cholangioplasty, nephrostomy, ureteral stents, chest tubes
Vascular Malformation
- Conditions: Arteriovenous malformation (AVM), Hereditary Hemorrhagic Telangiectasia (HHT)
- Services: Angiography, embolization
Pain Management
- Conditions: Knee pain from osteoarthritis, osteoporotic/pathologic spine fractures
- Services: geniculate artery embolization, vertebral augmentation (for example, kyphoplasty), soft tissue and bone ablation
Other Nonvascular Services
- Conditions: Abscess, pleural effusion, malnutrition, intestinal leak, pancreas leak, fistulae, benign thyroid nodules
- Services: Imaging-guided drainage, feeding tube placement and management, thyroid nodule ablation
Who we partner with
- Patients and their families
- Researchers from our own and other institutions
- Donors and other visionaries committed to improving the lives of others
- Referring colleagues in the field of liver transplant surgery
Who we are
- Faculty members
- Postdoctoral fellows
- Research staff
- Medical and graduate students
- Nurse practitioners
- Practice Managers